SHORT CASE- FINAL PRACTICAL GENERAL MEDICINE
NAME : R AKHIL CHANDRA
HALLTICKET NO : 1701006149
BATCH : 2017
This is an E log book to discuss our patient's de-identified health data shared after taking his guardian's signed informed consent. Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable comments in comment box are most welcomed.
Chief Complaints:-
A 47 year old female tailor by occupation resident of nalgonda came to the OPD with the chief complaints of:
* Fever since 3 months
* Facial rash since 10 days
HISTORY OF PRESENT ILLNESS:-
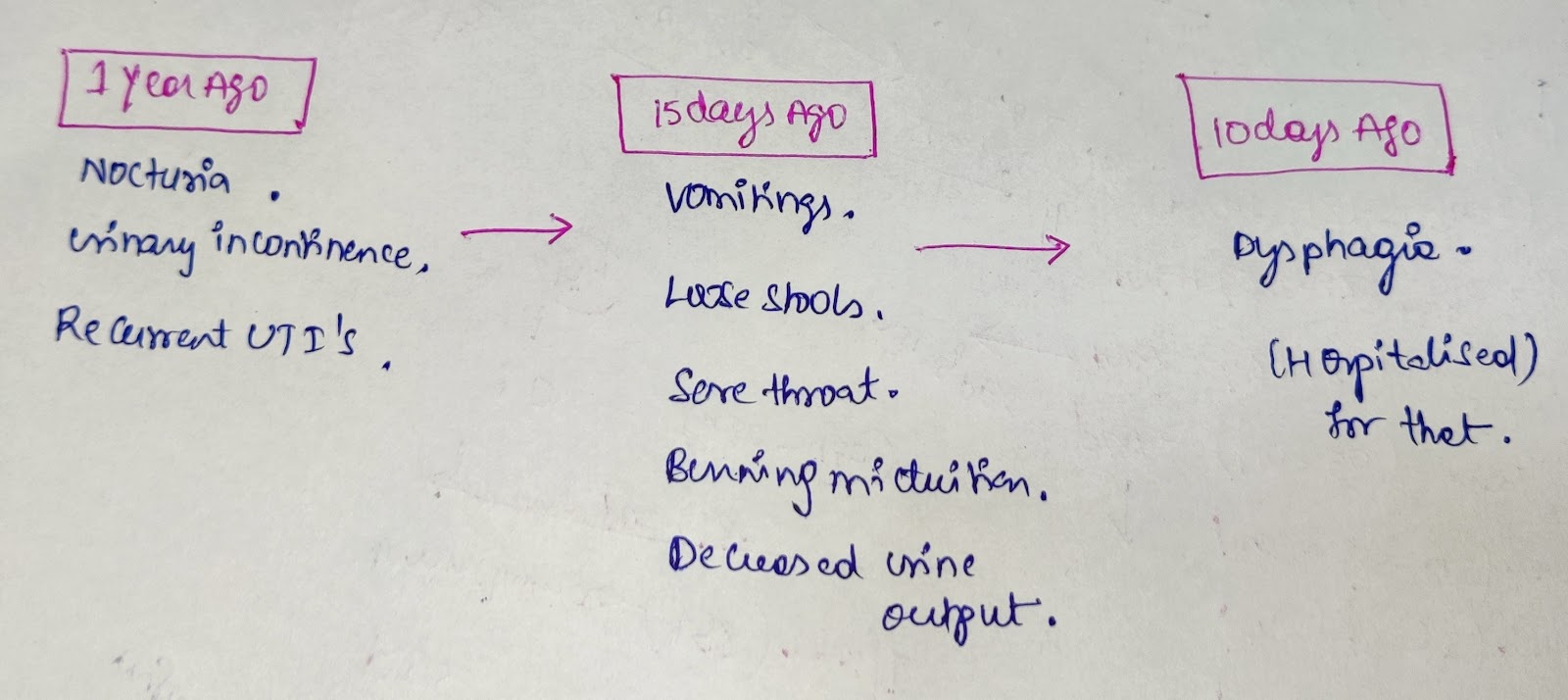
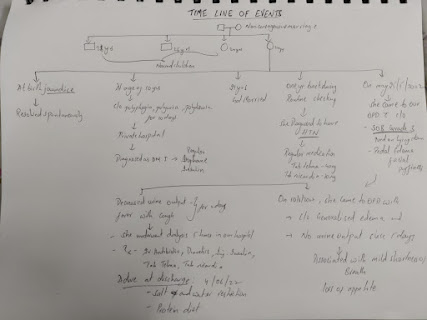
* Patient was apparently asymptomatic 10 years ago then she developed joint pains first in the both knees and ankles followed by both the hands. There was swelling associated with pain morning stiffness for about 15mins associated with limitation of movements. For this the patient was treated in private hospital and was tested RA POSITIVE and was on diclofenac, remained asymptomatic for 8 months,
* Last year at around month of August patient took covid vaccination of one dose following which she developed post vaccination joint pains.
* In the month of November patient consulted orthopedic and was given medication and thus relieved from symptoms.
* 3months back she developed fever which was Insidious in onset Intermittent on and off, not associated with chills and rigor. It was relieved on medication . She went to the private hospital but the fever was recurrent associated with abdominal pain came here 5 days back.
* 1 month back patient had an episode of loss of consciousness associated with sweating after taking metformin tablet prescribed by local RMP
* Patient also had facial rash over the face which increased on exposure to sun. It was a diffuse erythematous lesion and hyperpigmented papules were noted over the bilateral cheek sparing nasolabial folds, following intake of unknown medication for abdominal pain
PAST HISTORY:-
* Patient had a history of gradual painless loss of vision since 2011and was certified as blind
* Not a known case of diabetes asthma Epilepsy thyroid tuberculosis and coronary artery disease.
* No similar complaints in the family
PERSONAL HISTORY:-
* Diet: Mixed
* APPETITE: Decreased
* SLEEP: Disturbed
* BOWEL AND BLADDER MOVEMENTS: Regular
* ADDICTIONS: No addiction
GENERAL EXAMINATION:-
Patient is conscious coherent co operative well oriented to time place and person, moderately built and moderately nourished and is examined with informed consent.
Pallor: present
No icterus, cyanosis, clubbing, lymphadenopathy, edema.
VITALS:-
PULSE :86BPM
BP:120/80mm hg
RR:16cpm
SPO2:98%at room air
LOCAL EXAMINATION:-
* There is swelling in the left lower Limb on the lateral aspect with itching
* Local rise of temperature and redness.
* Pigmentation is seen and swelling was associated with pain which is throbbing in nature non radiating type
* No aggravating or relieving factors.
* Dorsalis pedis artery is felt.
* Erythematous rash is present on the cheek bilaterally. It is not associated with itching now.
* 10days back there was itching which gradually subsided.


SYSTEMIC EXAMINATION
CVS:-
INSPECTION: Shape of chest in normal
no visible neck veins
No rise in JVP
No visible pulsation scars.
PALPATION: All inspectory findings are confirmed.
Cardiac impulse felt at 5ty intercostal space 1cm medial to the mid clavicular line.
PERCUSSION: shows normal heart borders
AUSCULTATION: S1 S2 heard no murmurs
CNS:-
Normal tone and power.
Sensory system : touch vibration proprioception normal.
MOTOR SYSTEM: Normal tone and power
REFLEXES: Right Left
BICEPS 2+ 2+
TRICEPS 2+ 2+
SUPINATOR 2+ 2+
KNEE 2+ 2+
CRANIAL NERVE EXAMINATION:-
2nd cranial nerve Right Left
Visual acuity Counting fingers positive
Direct light reflex present. Present
Indirect light reflex present. Present
Perception of light Present. Present
Remaining cranial nerves normal.
GIT SYSTEM:-
INSPECTION: normal scaphoid abdomen with no pulsations and scars
PALPATION: inspectory findings are confirmed
no organomegaly, non tender and soft
PERCUSSION: normal resonant note present, liver border normal
AUSCULTATION: normal abdominal sounds heard, no bruit present
RESPIRATORY SYSTEM:
INSPECTION: Shape of chest is elliptical,
B/L symmetrical chest,
Trachea in central position,
Expansion of chest- left normal
Right - decreased
PALPATION: All inspectory findings are confirmed,
No tenderness, No local rise of temperature,
trachea is deviated to the right,
Tactile vocal fremitus: decreased on right side ISA, InfraSA, AA, IAA.
PERCUSSION: Dull note present in right side ISA, InfraSA, AA, IAA.
AUSCULTATION: B/L air entry present, vesicular breath sounds heard
Decreased intensity of breath sounds in right SSA,IAA
INVESTIGATIONS:-
ANA REPORT:

HEMATOLOGY:
IMPRESSION: Normocytic hypochromic ( Hb 6.0 )
Mild decrease in Platelet count
Relative monocytosis


PROVISIONAL DIAGNOSIS:
SECONDARY SJOGRENS SYNDROME
LEFT LOWER LIMB CELLULITIS WITH BILATERAL OPTIC ATROPHY
TREATMENT:
1.INJ PIPTAZ 4.5 gm IV/ TID.
2.INJ METROGEL100 ML IV/TID
3.INJ NEOMOL1GM/IV/SOS
4.TAB CHYMORAL FORATE PO/TID
5.TAB PAN 40 MG PO/ OD.
6.TAB TECZINE10 MG PO/OD
7.TAB OROFERPO/OD.
8.TAB HIFENAC-P PO/OD
9HYDROCOTISONE cream 1%on face for 1week
Comments
Post a Comment