general medicine assignment 178Akhilchandra
GENERAL MEDICINE ASSIGNMENT
1)Pulmonology;
A)
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
1Q) what is the evolution of the symptomatology in this patient interms of an event timeline and where is the anatomical localisation for the problem and what is the primary etiology of the patient problem ?
Ans :Evolution of symptomatology ;
1st episode of SOB - 20 yr back lasted 1week approximately
2nd episode of SOB - 12 yr back lasted for 20 days
From then she has been having yearly episodes for the past 12 yrs lasting around a month
8 years ago she was diagnosed with diabetes
Anemia 5 years ago
Generalisedweakness - 1 month back
Diagnosedwith hypertension - 20 days back
pedaledema - 15 days back
Facialpuffiness- 15 days back
Anatomical location of problem - lungs
Primary etiology of patient- usage of chulha since 20 yrs
2Q)what r the mechanism of action indication and efficacy over placebo of each of the phramacological and nonphramacological interventions used for this patient?
2Ans)~Head end elevation :
MOA ;
improves oxygenation
decreasesincidence VAP
increaseshemodynamic performance
Increasesend expiratory lung volume
decreases incidence of aspiration
Indication::head injury
meningitis
pneumonia
oxygen inhalation to maintain spo2
Bipap:non invasive method
MOA :assist ventilation by delivering positive expiratory and inspiratory pressure with out need for ET incubation9
3. Cause for current acute excerbation -infection
4.could the ATT affected her symptoms if so how?
Yes,
Isoniazidand rifampcin -nephrotoxic - raised RFT was seen
Neurology
2.A)
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
1) what is the evolution of the symptomology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans: Evolution of symptomatology;
2-3 episodes of seizures
1st episode -1 year back
Recent episode of seizure 4 months back
Following cessation of alcohol for 24
It was associated with restlessness, sweating, tremors.
Decrease in food intake since 9days
Primary etiology of pt problem: Alcohol intake
2)what are the mechanism of action, indication, and efficacy over placebo of each of the pharmacological and nonpharmacological interventions used for this patient?
Ans:
1. Inj.Thiamine as a supplement to cope with thiamine deficiency
2.IVF NS&RL-source of electrolytes & water
For dehydration,hypovolemia , increase plasma volume
3.inj.lorazepam-Lorazepam binds to benzodiazepine receptors on the postsynaptic GABA-A ligand-gated chloride channel neuron at several sites within the central nervous system.it enhances the inhibitory effects of GABA, which increases the conductance of chloride ions into the cell
4.pregabalin subtly reduces the synaptic release of several neurotransmitters, apparently by binding to alpha2-delta subunits, and possibly accounting for its actions invivo to reduce neuronal excitability and seizures.
5.Lactulose is used in preventing and treating clinical portal-systemic encephalopathy .its chief mechanism of action is by decreasing the intestinal production and absorption of ammonia.
6.Potchlor liquid is used to treat low levels of potassium in the body.
3)why have neurological symptoms appeared this time, that were absent during withdrawal earlier ? what could be a possible cause for this time?
Ans:
Due to excess thiamine deficiency and excess toxins accumulation due to renal disease caused by excess alcohol addiction.
4)what is the reason for giving thiamine in this patient?
ANS ;
Thiamine maintains membrane integrity & osmotic gradients across cell membranes
chronic alcohol consumption causes thiamine deficiency due to impaired absorption of thiamine from the intestine,Thiamine, one of the first B vitamins to be discovered also known as Vitamin B1, is a coenzyme that is essential for intricate organic pathways and plays a central role in cerebral metabolism. This vitamin acts as a cofactor for several enzymes in the Krebs cycle and the pentose phosphate pathway, including alpha-keto-glutamic acid oxidation and pyruvate decarboxylation. Thiamine-dependent enzymes function as a connection between glycolytic and citric acid cycles. Therefore, deficiency of thiamine will lead to decreased levels of alpha-keto-glutarate, acetate, citrate, acetylcholine, and accumulation of lactate and pyruvate. This deficiency can cause metabolic imbalances leading to neurologic complications
5)what is the probable cause for kidney injury in this patient?
Ans;
Alcohol can affects renal functions such as filtration of blood, regulation of body fluids.
alcohol could be cause of kidney injury
6)what is the probable cause for the normocytic anaemia?
Ans;
Alcohol can affect iron metabolism,reduces iron absorption form intestines,also affects the Bonemarrow causing decrese in count of RBC,WBC
7)could chronic alcohlism have aggravated the foot ulcer formation ?if yes and why ?
Ans;
yes,As the patient is diabetic the chance of ulcer formation increases .in a patient of chronic alcoholic patient's immune system is weak healing of an ulcer is slow.
2. B)
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
1) What is the evolution of the symptomology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patients problem?
ANS. 7 days back giddiness that started around 7 in the morning associated with one episode of vomiting, giddiness subsided upon taking rest.
4 days back he developed giddiness that was sudden onset, continuous and gradually progressive. It increased on standing and while walking.
H/O postural instability- falls while walking
Associated with bilateral hearing loss, aural fullness, presence of tinnitus
Associated vomiting- 2-3 episodes per day, non projectile, non bilious without food particles
Present day of admission- Slurring of speech, deviation of mouth that got resolved the same day
Anatomical location- There is a presence of an infarct in the inferior cerebellar hemisphere of the brain.
Etiology- Ataxia is the lack of muscle control or co-ordination of voluntary movements, such as walking or picking up objects. This is usually a result of damage to the cerebellum.
In this case, the patient has hypertension for which he has been prescribed medication that he has not taken. Stroke due to an infarct can be caused by blockade or bleeding in the brain due to which blood supply to the brain is decreased, depriving it of essential oxygen and nutrients. This process could’ve caused the infarct formation in the cerebellar region of the brain, thus causing cerebellar ataxia.
2) What are the mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
ANS.
A) Tab Vertin 8mg- This is betahistine, which is an anti- vertigo medication
MOA- It is a weak agonist on H1 receptors located on blood vessels of the inner ear. This leads to local vasodilation and increased vessel permeability. This can reverse the underlying problem.
Indications- Prescribed for balance disorders. In this case it is used due to patients history of giddiness and balance issues.
B) Tab Zofer 4mg- This is ondanseteron- It is an anti emetic
MOA- It is a 5H3 receptor antagonist on vagal afferents in the gut and they block receptors even in the CTZ and solitary tract nucleus.
Indications- Used to control the episodes of vomiting and nausea in this patient.
C) Tab Ecosprin 75mg- This is aspirin. It is an NSAID
MOA- They inhibit COX-1 and COX-2 thus decreasing the prostaglandin level and thromboxane synthesis
Indications- They are anti platelet medications and in this case used to prevent formation of blood clots in blood vessels and prevent stroke.
D) Tab Atorvostatin 40mg- This is a statin
MOA- It is an HMG CoA reductase inhibitor and thus inhibits the rate limiting step in cholesterol biosynthesis. It decreases blood LDL and VLDL, decreases cholesterol synthesis, thus increasing LDL receptors in liver and increasing LDL uptake and degeneration. Hence plasma LDL level decreases.
Indications- Used to treat primary hyperlipidemias. In this case it is used for primary prevention of stroke.
E) Clopidogrel 75mg- It is an antiplatelet medication
MOA- It inhibits ADP mediated platelet aggregation by blocking P2Y12 receptor on the platelets.
Indications- In this case it decreases the risk of heart disease and stroke by preventing clotting
F) Thiamine-
The patient consumes excess alcohol causes thiamine deficiency
Indications- Given to this patient mainly to prevent Wernickes encephalopathy- that can lead to confusion, ataxia and opthalmoplegia.
G) Tab MVT- This is methylcobalamin
Mainly given in this case for vitamin B12 deficiency.
3) Did the patients history of denovo hypertension contribute to his current condition?
ANS. Yes
A cerebellar infarct is usually caused by a blood clot obstructing blood flow to the cerebellum. High blood pressure that is seen in hypertension (especially if left untreated) can be a major risk factor for the formation of cerebellar infarcts.
Increased shear stress is caused on the blood vessels. The usual adaptive responses are impaired in this case, thus leading to endothelial dysfunction in this case. High BP can also promote cerebral small vessel disease. All these factors contribute to eventually lead to stroke.
4) Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic stroke?
ANS.
Yes, The patient has history of chronic alcoholism and susceptible to ischemic stroke.
2. C) http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
10 years back-Paralysis of both upper and lower limbs (bilateral)
1 year back-Right and left paresis due to hypokalemia
8 months backSwelling over legs
7 months back - blood infection
2 months back- neck pain
6 days back- pain along left upper limb
5 days back- chest pain, SOB
Anatomical localization: Cervical spine
Dehydrated disks. Disks act like cushions between the vertebrae of your spine. By the age of 40, most people's spinal disks begin drying out and shrinking, which allows more bone-on-bone contact between the vertebrae.
Bone spurs. Disk degeneration often results in the spine producing extra amounts of bone in a misguided effort to strengthen the spine. These bone spurs can sometimes pinch the spinal cord and nerve roots.
Herniated disks. Age also affects the exterior of your spinal disks. Cracks often appear, leading to bulging (herniated) disks — which sometimes can press on the spinal cord and nerve roots.
Stiff ligaments. Ligaments are cords of tissue that connect bone to bone. Spinal ligaments can stiffen with age, making your neck less flexible.
2) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
The primary hypokalemic periodic paralysis is exacerbated by strenuous exercise, high carbohydrate diet, cold and excitement, which was not found in this case. secondary periodic hypokalemic paralysis have been reported in association with gastroenteritis, diuretic abuse, renal tubular acidosis, Bartter syndrome, villous adenoma of colon, and hyperthyroidism.
Risk factors ;
Female
Medications like diuretics
Heart failure
Hypertension
Low BMI
cushing syndrome
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
Inversion of T waves -mild hypokalemia,
followed by Q-T interval prolongation
visible U wave and mild ST depression.
2 D)
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
QUESTIONS:
1.Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
seizures after ischaemic strokes. An increase in intracellular Ca2+ and Na+ with a resultant lower threshold for depolarisation, glutamate excitotoxicity, hypoxia, metabolic dysfunction, global hypoperfusion, and hyperperfusion injury
Seizures after haemorrhagic strokes are thought to be attributable to irritation due to (hemosideri. Deposits)caused by products of blood metabolism
Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.
2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Initially the patient might have had Simple partial seizures (no loss of consciousness) and might have progressed to Generalised Tonic Clonic seizures ,loss of consciousness in progressed GTCS.
E)
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
Questions: 1) What could have been the reason for this patient to develop ataxia in the past 1 year?
The patient has minor unattended head injuries in the past 1 yr. Accoding to the CT scan, the patient has cerebral haemorrhage in the frontal lobe causing probably for the occurrence of Frontal love ataxia
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
The patient has minor unattended head injuries. During the course of time the minor hemorrhages if present should have been cured on their own. But the patient is a chronic alcholic. This might have hindered the process of healing or might have stopped the healing rendering it to grow further more into 13 mm sized hemorrhages occupying Frontal Parietal and Temporal lobes
F)
http://shivanireddymedicalcasediscussion.blogspot.com/2021/05/a-30-yr-old-male-patient-with-weakness.html
Questions
1.Does the patient's history of road traffic accident have any role in his present condition?
The closeness of facial bones to the cranium would suggest that there are chances of cranial injuries. Since the Zygomatic arch and Mandibular process is very close to the cranium, this might play a role in the patient's present condition
2.What are warning signs of CVA?
Weakness or numbness of the face, arm or leg, usually on one side of the body
Trouble speaking or understanding
Problems with vision, such as dimness or loss of vision in one or both eyes
Dizziness or problems with balance or coordination
Problems with movement or walking
Fainting or seizure
Severe headaches with no known cause, especially if they happen suddenly
3.What is the drug rationale in CVA?
Mannitol- Because of its osmotic effect, mannitol is assumed to decrease cerebral edema. Mannitol might improve cerebral perfusion by decreasing viscosity, and as a free-radical scavenger, it might act as a neuroprotectant.
Ecospirin
It for management of heart attack, stroke, heart conditions such as stable or unstable angina (chest pain) due to a blood clot.
Atrovas-Atorva 40 it is a statin, used to lower cholesterol and to reduce the risk of heart diseases.
Rt feed RT feed is a nursing procedure to provide nutrition to those people who are either unable to obtain nutrition by mouth or are not in a state to swallow the food safely.
4. Does alcohol has any role in his attack?
When the patient met with an accident there might be cranial damage which was unnoticed.
If so his occasional drinking may or may not have hindered the process of the minor hemorrhages getting healed and might have caused this condition
But since the patient is not a chronic alcoholic and so Alcohol might not have played any role.
Therefore it cannot be evaluated without further details
5.Does his lipid profile has any role for his attack??
The inverse relationship between serum HDL-C and stroke risk . When taken together it seems clear that higher baseline levels of serum HDL-C lower the risk of subsequent ischemic stroke.
2.G)
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
a)what is myelopathy hand?
There is loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and release rapidly with these fingers. These changes have been termed "myelopathy hand" and appear to be due to pyramidal tract involvement.
b)what is finger escape?
Finger eacape(Wartenberg's sign )is a neurological sign consisting of involuntary abduction of the fifth (little) finger, caused by unopposed action of the extensor digiti minimi. . This finding of weak finger adduction in cervical myelopathy is also called the "finger escape sign".
c)what is Hoffman's sign?
Hoffman's sign or reflex is a test used to examine the reflexes of the upper extremities. This test is a quick, equipment-free way to test for the possible existence of spinal cord compression from a lesion on the spinal cord or another underlying nerve condition
2 H)
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
1) What can be the cause of her condition ?
Ans ;Could be IRON DEFICENCY ANEMIA.
2) What are the risk factors for cortical vein thrombosis?
Ans: Risk factors ;
Pregnancy
antiphospholipid syndrome
protein C and S deficiency
antithrombin III deficiency
factor V mutation
Cancer
Collagen vascular diseases like lupus, Wegener’
Obesity
Intracranial hypotension
Inflammatory bowel disease
Sickle cell anemia
Chronic hemolytic anemia
Beta-thalassemia major
Heart disease
Iron deficiency
Certain infections
Dehydration
Head injury
3)There was seizure free period in between but again sudden episode of GTCS why?resolved spontaneously why?
Ans: there was a sezuire free period due to administration of antiepileptic drugs as the effect of drugs weans off the sezures appear again followed by administration of phenobarbitone leading to spontaneous resolution of the sezuires.
4) What drug was used in suspicion of cortical venous sinus thrombosis?
Ans: heparin as CLEXANE was given to relive clot in suspission of CVST
3. Cardiology
A)
https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html
https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html
1.What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction?
Ans:Preserved ejection fraction (HFpEF) – also referred to as diastolic heart failure. The heart muscle contracts normally but the ventricles do not relax as they should during ventricular filling (or when the ventricles relax).
Reduced ejection fraction (HFrEF) – also referred to as systolic heart failure
HFpEF is preceded by chronic comorbidities, such as hypertension, type 2 diabetes mellitus (T2DM), obesity, and renal insufficiency, whereas HFrEF is often preceded by the acute or chronic loss of cardiomyocytes due to ischemia, a genetic mutation, myocarditis, or valvular disease
2.Why haven't we done pericardiocenetis in this pateint?
Ans: Pericardiocentesis is not done here Because the effusion was self healing ,It reduced from 2.4cm to 1.9 cm.
3.What are the risk factors for development of heart failure in the patient?
Ans: risk factors for development of heart faliure in this patent
Alcohol abuse increases the risk of atrial fibrillation, heart attack and congestive heart failure
high blood pressure
Smoking
Diabetes
AV block can be associated with severe bradycardia and hemodynamic instability. It has a greater risk of progressing to third-degree heart block .
wosening of pericardial effusion leaing to cardiac tamponade.
4.What could be the cause for hypotension in this
Ans : visceral pericardium may have thickened which is restricting the heart to expand causing hypotension
B)
https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html
https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html
QUESTIONS
1)What are the possible causes for heart failure in this patient?
Ans;
The patient was diagnosed with type 2 diabetes mellitus 30 years ago.
uncontrolled diabetes which is major risk factor for heart failure
The patient was also diagnosed with hypertension 19 yrs. ago which is also a risk factor for heart failure
He is a chronic alcoholic since 40 years which is a risk factor for heart failure could be the cause of heart failure
The patient was diagnosed with chronic kidney disease stage,also the risk factors for heart failure
2)what is the reason for anaemia in this case?
The patient has normocytic normochromic anaemia. it could be anaemia of a chronic disease as the patient is diagnosed with CKD stage IV.
Chronic kidney disease results in decreased production of erythropoietin which in turn decreases the production of red blood cells from the bone marrow.
Patient’s with anaemia and CKD also tend to have deficiency in nutrients like iron, vitamin B12 and folic acid essential in making healthy red blood cells
3) What is the reason for blebs and non-healing ulcer in the legs of this patient?
Diabetes mellitus. CKD is also known to cause delay in healing of wounds along with poorly controlled diabetes. Anaemia can also slow down healing of ulcer
4) What sequence of stages of diabetes has been noted in this patient?
There are 4 stages in type 2 diabetes- insulin resistance, prediabetes, type 2 diabetes and
vascular complications, including retinopathy, nephropathy , related microvascular events.
The patient is diagnosed with diabetic triopathy exhibiting sequence of neuropathy, retinopathy and nephropathy
The patient has been diagnosed with diabetic retinopathy, CKD stage IV and shows signs of diabetic neuropathy such as numbness.
C)
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans: Facial puffiness 3 yrs back
Sob grade 2 -1yr ago
Sob grade 2- 2days back again
Sob grade 4
Decreased urine output since 2 days
Anuria (since morning)
Anatomical site: blood vessels
2. What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans:
Tab.Dytor
Its antagonising effect of aldosterone &sprironolactone it helps to prevent potassium loss
Tab .Acitrom
It inhibits an enzyme vit.k epoxide reductase
Dobutamine-increases cardiac output
Indications are cardiogenic shock , Reversible heart failure
Digoxin-Positive Ionotropic: It increases the force of contraction of the heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump, an enzyme that controls the movement of ions into the heart.
Indications are Atrial fibrillation ,atrial flutter,Heart failure,Abortion
3.What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?
Ans: stage 3 cardio renal syndrome
4. What are the risk factors for atherosclerosis in this patient?
Ans: Hypertension.
5. Why was the patient asked to get those APTT, INR tests for review?
And: Because of Thrombosis and to check on development of thrombosis.
D)
https://daddalavineeshachowdary.blogspot.com/2021/05/67-year-old-patient-with-acute-coronary.html?m=1
Questions:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Answer ; Evolution of symptomatology
diabetes since 12 years
Pulmonary TB 7monthsback hypertension since 6 months.
Anatomical localisation of problem; cardiovascular system
Etiology- patient is hypertensive &diabetic can develop atherosclerosis.
MI can occur due to decreased myocardial oxygen supply due to severe coronary artery narrowing or acute atherosclerotic plaque rupture/erosion and superimposed thrombus formation. Due to decrease in myocardial oxygen supply there is heartburn Due to heart muscle damage there is decrease in the pump function of left ventricle causing decrease in pulmonary circulation which leads to shortness of breathe (dyspnea). It occurs due to partial occlusion of a major vessel or a complete occlusion of a minor vessel .
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Answer ;
1.Met Xl -metoprolol is a cardio selective beta blocker improves blood flow
Indicated in angina,high BP
2.non-pharmacological intervention advised to pt;
Percutaneous coronary intervention
Antiplatelet therapy- aspirin+ticagrelor aspirin daily improves survival, reduces risk of mortality, MI, stroke ticagrelor reduces recurrent ischaemic events. Glycoprotein II b /III a receptor antagonists- tirofiban , abciximab block the final common pathway of platelet aggregation and are potent inhibitors of platelet-rich thrombus formation Anticoagulants- heparin reduces the risk of thromboembolic complications and prevents re-infarction.
3) What are the indications and contraindications for PCI?
Indications- ST-elevation MI
atypicalchest pain,
stablee angina,
unstable angina,
positivee stress test Non ST-elevation Mi
Contraindications- Intolerance to oral antiplatelets
Hypercoagulable state
Chronic kidney disease
Lackk of cardiac support Coagulopathy Hypercoagulable states Critical left main coronary stenosis without collateral flow from a native vessel or previous bypass graft to the left anterior descending artery Diffusely diseased vessel without focal stenosis A single diseased vessel providing all perfusion to the myocardium Total occlusion of a coronary artery Stenosis <50%
4) What happens if a PCI is performed in a patient who does not need it? What are the harms of overtreatment and why is research on overtesting and overtreatment important to current healthcare systems?
Ans; bleeding,blood vessels damage, allergic reaction to dye, Arrhythmia
Complications- Acute; occlusion of target vessels or a side branch by thrombus or a loose flap of intima (coronary artery dissection), and consequent myocardial damage Long term complication; re-stenosis
E) https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans;
Evolution of symptomatology:
Uncontrolled DM2 since 8 years
Mild chest pain -days back
Anatomical localisation: Inferior wall of heart
Primary etiology: uncontrolled DM-2
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans;
TAB. ASPIRIN
MOA; COX inhibitor. This prevents the production of pain-causing prostaglandins.
TAB ATORVAS
Atorvastatin(statins)cholesterol lowering agent
TAB CLOPIBB 300mg PO/STAT
MOA;clopidogrel inhibits platelet aggregation & clot formation
3) Did the secondary PTCA do any good to the patient or was it unnecessary?
Ans; Yes,it is safe and for management for recurrence of stenosis after initially successful angioplasty.
https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
4) Gastroenterology
4 A) https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-pancreatitis-with.html
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-pancreatitis-with.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
A: Evolution of symptomatology;
One episode of vomiting & pain per abdomen 5years back
5-6episodes of vomiting in past 1 year
Pain per abdomen since 4 days in left hypochondriac,lumber, hypogastric regions
Constipation since 4 days
Burning micturition since 4 days
antomical location of problem is pancreas
2) What is the efficacy of drugs used along with other non pharmacological treatment modalities and how would you approach this patient as a treating physician?
PHARMACOLOGICAL INTERVENTIONS
ING. MEROPENEM
Meropenem inhibits bacterial cell wall synthesis like other β-lactam antibiotics. In contrast to other beta-lactams, it is highly resistant to degradation by β-lactamases or cephalosporinases.
2) ING. METROGYL
MOA:Metronidazole inhibits protein synthesis of organism by interacting with DNA and causing a loss of helical DNA structure and strand breakage. Therefore, it causes cell death in susceptible organisms.
3) ING. AMIKACIN
MOA; aminoglycoside, It binds to bacterial 30S ribosomal subunits and interferes with mRNA binding and tRNA acceptor sites, interfering with bacterial growth.
4) TPN ( Total Parenteral Nutrition )
mechanism: early administration of enteral nutrition must be the standard therapeutic approach in patients with severe acute pancreatitis it decreases the risk of infection; TPN is only required in a few patients.
5) IV NS / RL
mechanism:Patients with acute pancreatitis lose a large amount of fluids to third spacing into the retroperitoneum and intra-abdominal areas. Accordingly, they require prompt intravenous (IV) hydration within the first 24 hours. Especially in the early phase of the illness, aggressive fluid resuscitation is critically important.
6) ING. OCTREOTIDE
Octreotide decreases the release of growth stimulating hormones, decreases blood flow to the digestive organs, and inhibits the release of digestive hormones such as serotonin, gastrin, vasoactive intestinal peptide, secretin, motilin, and pancreatic polypeptide.
Octreotide is useful in overdose management of sulfonylurea type hypoglycemic medications, when recurrent or refractory to parenteral dextrose. Mechanism of action is the suppression of insulin secretion.
7) ING. PANTOP
MOA; inhibit the gastric acid production. In the gastric parietal cell of the stomach, pantoprazole covalently binds to the H+/K+ ATP pump to inhibit gastric acid and basal acid secretion.
8) ING. THIAMINE
mechanism:Vitamin B1 (thiamin) is indispensable for normal function/health of pancreatic cells due to its critical role in oxidative energy metabolism, ATP production, and in maintaining normal cellular redox state.
9) ING. TRAMADOL
MOA; Analgesic
B) https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
1) What is causing the patient's dyspnea? How is it related to pancreatitis
Ans;The cause of dyspnea might be pleural effusion
2) Name possible reasons why the patient has developed a state of hyperglycemia
Ans:
hyperglycemia could thus be due to hyperglucagonemia secondary to stress
Due to decreased synthesis and release of insulin secondary to the damage of pancreatic β-cells
elevated levels of catecholamines and cortisol
3) What is the reason for his elevated LFTs? Is there a specific marker for Alcoholic Fatty Liver disease?
Ans;
LFT are increased due to hepatocyte injury
increase in ALT levels can be a sign of liver damage.
elevated alanine transaminase (ALT) and aspartate transaminase (AST), usually one to four times the upper limits of normal in alcoholic fatty liver.
4) What is the line of treatment in this patient?
Treatment:
• IVF: 125 mL/hr
• Inj PAN 40mg i.v OD
• Inj ZOFER 4mg i.v sos
• Inj Tramadol 1 amp in 100 mL NS, i.v sos
•Tab Dolo 650mg sos
• GRBS charting 6th hourly
• BP charting 8th hourly
C) https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
1) What is the most probable diagnosis in this patient?
As;
The most probable diagnosis is abdominal hemorrhage.
This will give reasoning to the abdominal distention, and the blood which is aspirated.
Differential Diagnosis:
-Ruptured Liver Abscess.
- Organized collection secondary to Hollow viscous Perforation.
-Organized Intraperitoneal Hematoma.
- Free fluid with internal echoes in Bilateral in the Subdiaphragmatic space.
-Grade 3 RPD of right Kidney
2) What was the cause of her death?
Cause of her death can be due to complications of laparotomy surgery ,
Patient underwent an emergency laparotomy surgery
Complications of emergency laparotomy;
hemorrhage , infection, or injury to internal organs.
3) Does her NSAID abuse have something to do with her condition? How?
NSAID-induced renal dysfunction: decreased glomerular perfusion
decreased glomerular filtration rate
acute renal failure.
Chronic NSAIDs use related to hepatotoxicity.
major adverse effects of NSAIDs ; gastrointestinal mucosa injury, NSAIDs have also been associated with hepatic side effects --hepatitis with jaundice ,fulminant liver failure.
5)NEPHROLOGY
A) https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
1.what could be the cause for his SOB
Ans- Due to Acidosis caused by Diuretics
2. Reason for Intermittent Episodes of drowsiness
Ans:Hyponatremia was the cause for intermittent episodes of drowsiness
3.why did he complaint of fleshy mass like passage in urine
Ans-fleshy mass like passage appeared to him bcz plenty of pus cells passes in his urine passage
4. What are the complications of TURP that he may have had
Ans-
1. Difficulty micturition
2. Electrolyte imbalances
3. Infection
B) https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
1.Why is the child excessively hyperactive without much of social etiquettes ?
ANS;The exact pathophysiology of Attention Deficit Hyperactivity Disorder (ADHD) is not clear. With this said, several mechanisms have been proposed as factors associated with the condition. These include abnormalities in the functioning of neurotransmitters, brain structure and cognitive function.
Due to the efficacy of medications such as psychostimulants and noradrenergic tricyclics in the treatment of ADHD, neurotransmitters such as dopamine and noradrenaline have been suggested as key players in the pathophysiology of ADHD.
Depressed dopamine activity has been associated with the condition
2. Why doesn't the child have the excessive urge of urination at night time ?
Ans:the child doesn’t have the excessive urge of urination at night time because ADHD is a physcosomatic disorder
3. How would you want to manage the patient to relieve him of his symptoms?
6) INFECTIOUS DISEASES
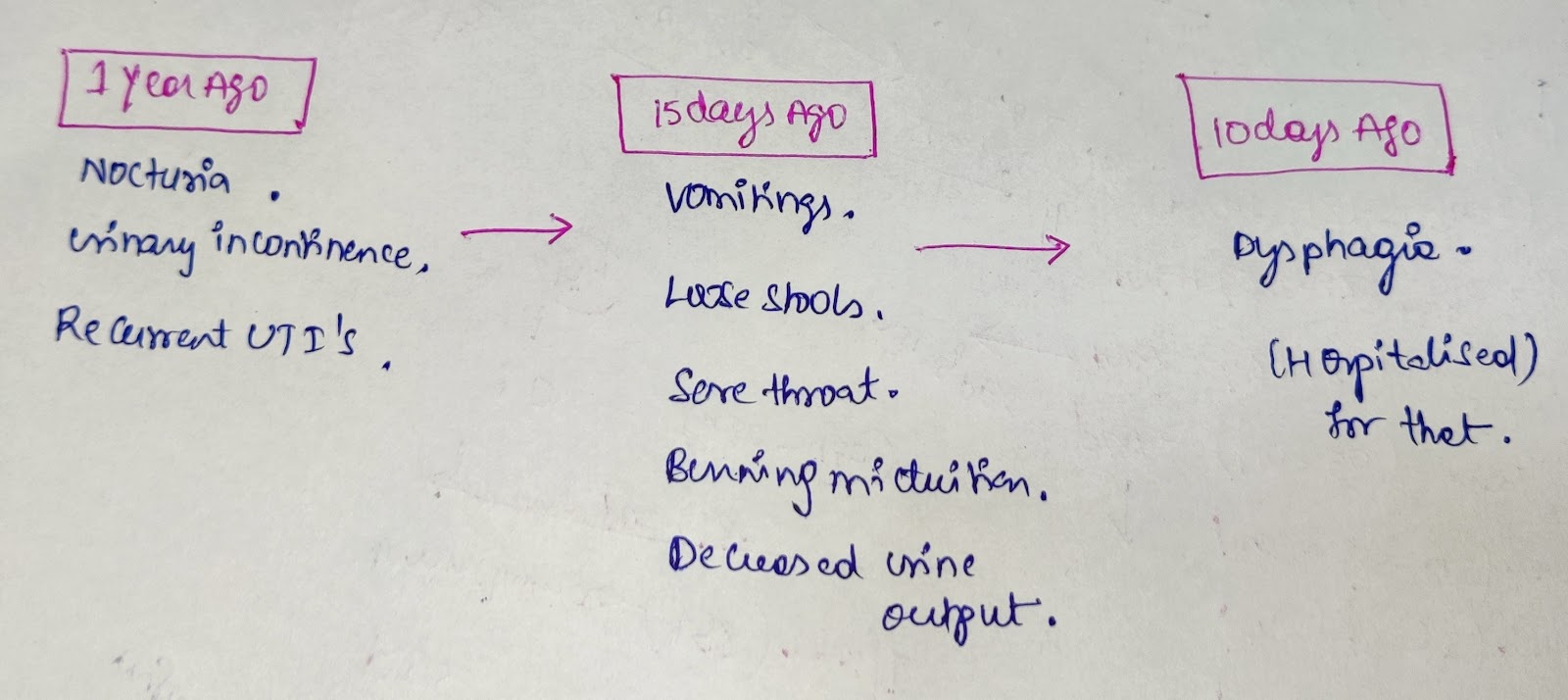
A) https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
1) Which clinical history and physical findings characteristic of tracheoesophageal fistula?
Ans;Cough on taking food&liquids
2)What are the chances of this patient developing immune reconstitution inflammatory syndrome(iris)??can we prevent?
Ans;immune reconstitution inflammatory syndrome (iris)occurs in 2 forms
1.unmasking IRIS refers to flareup of an underlying, previously undiagnosed infection soon after anti retroviral therapy (ART)
2.paradoxical IRIS refers to worsening of a previously treated infection after ART is started
Patients with mycobacterial diseases at the time of ART are at higher risk of developing IRIS.
Prevention;
Initiation of ART before development of advanced immunosupression.
7) INFECTIOUS DISEASES &HEPATOLOGY
A) https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
1)Do you think drinking locally made alcohol cause liver abscess in this patient due to predisposing factors present in it ? What could be the cause in this patient?
Ans; yes, it could be due to intake of contaminated toddy in this patient
2)what is the etiopathogenesis of liver abscess in a chronic alcoholic patient?
Ans ; Alcohol is a predisposing factor for the formation of liver abscesses that is both amoebic as well as pyogenic liver abscess . It is also proven that Alcoholism is never an etiological factor for the formation of liver abscess.
3)is liver abscess is more common in right lobe?
Ans;yes ,right lobe is involved due to its more blood supply to it
4Q) what r the indications for USG guided aspiration of liver abscess
Ans- Indications for USG guided aspiration of liver abscess;
1. Large abscess more than 6cms
2. Left lobe abscess
3.Caudate lobe abscess
4. Abscess which is not responding to drugs
B) https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
1) Cause of liver abcess in this patient ?
Ans; Entamoeba Histolytica
2) How do you approach this patient ?
Ans:APPROACH IN THE PATIENT OF AMOEBIC LIVER ABCESS
3) Why do we treat here ; both amoebic and pyogenic liver abcess
Ans:we treat the paient for both amoebic and pyogenic abcess so that we dont rely only on anti-amebic therapy and insure comple treatment of the cause
4) Is there a way to confirm The definitive diagnosis in this patient?
Ans:
Serologic testing is the most widely used method of diagnosis for amebic liver abscess. In general, the test result should be positive, even in cases when the result of the stool test is negative
The diagnosis of amebic liver abscess was based on four or more of the following criteria:
1. a space-occupying lesion in the liver diagnosed by ultrasonography and suggestive of abscess,
2. clinical symptoms ;fever, pain in the right hypochondrium , lower chest, back, or tip of the right shoulder),
3.enlarged and/or tender liver, usually without jaundice,
4.raised right dome of the diaphragm on chest radiograph, and
5.improvement after treatment with antiamebic drugs -metronidazole
8) INFECTIOUS DISEASE
A) http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary aetiology of the patient's problem?
3 years ago- diagnosed with hypertension
21 days ago- received vaccination at local PHC which was followed by fever associated with chills and rigors, high grade fever, no diurnal variation which was relieved on medication
18 days ago- complained of similar events and went to the the local hospital
11 days ago - Generalized weakness and facial puffiness and periorbital oedema. Patient was in a drowsy state
4 days ago-
a. patient presented to casualty in altered state with facial puffiness and periorbital oedema and weakness of right upper limb and lower limb
b. towards the evening patient periorbital oedema progressed
c. serous discharge from the left eye that was blood tinged
d. was diagnosed with diabetes mellitus
patient was referred to a government general hospital
patient died 2 days ago
patient was diagnosed with diabetic ketoacidosis and was unaware that he was diabetic until then. This resulted in poorly controlled blood sugar levels. The patient was diagnosed with acute oro rhino orbital mucormycosis . rhino cerebral mucormycosis is the most common form of this fungus that occurs in people with uncontrolled diabetes
the fungus enters the sinuses from the environment and then the brain.
The patient was also diagnosed with acute infarct in the left frontal and temporal lobe. Mucormycosis is associated with the occurrence of CVA
2)What is the efficacy of drugs used along with other non-pharmacological treatment modalities and how would you approach this patient as a treating physician?
The proposed management of the patient was –
1. inj. Liposomal amphotericin B according to creatinine clearance
2. 200mg Iitraconazole was given as it was the only available drug which was adjusted to his creatinine clearance
3. Deoxycholate was the required drug which was unavailable
along with the above mentioned treatment for the patient managing others symptoms is also done by-
I. Management of diabetic ketoacidosis –
(a) Fluid replacement- The fluids will replace those lost through excessive urination, as well as help dilute the excess sugar in blood.
(b) Electrolyte replacement-The absence of insulin can lower the level of several electrolytes in blood. Patient will receive electrolytes through a vein to help keep the heart, muscles and nerve cells functioning normally.
(c) Insulin therapy- Insulin reverses the processes that cause diabetic ketoacidosis. In addition to fluids and electrolytes, patient will receive insulin therapy
3Q) What are the postulated reasons for a sudden apparent rise in the incidence of mucormycosis in India at this point of time?
Mucormycosis is may be being triggered by the use of steroids, a life-saving treatment for severe and critically ill Covid-19 patients. Steroids reduce inflammation in the lungs for Covid-19 and appear to help stop some of the damage that can happen when the body's immune system goes into overdrive to fight off coronavirus. But they also reduce immunity and push up blood sugar levels in both diabetics and non-diabetic Covid-19 patients.

Comments
Post a Comment